

HYPERKALAEMIA
Hyperkalaemia is a condition in which serum level is above 5.5 mmol/L . If serum level is more than 6.5 mmol / 1 requires urgent treatment because of the risk of cardiac complications. The following changes can occur in ECG .
• Tall tented T wave +_ Flat p- wave +_ increased p.R interval .
• Widening of the QRS complex.
CAUSES :
Primary renal disease
⁃ Acute renal failure
⁃ Chronic renal failure
⁃ Type IV Renal tubular acidosis
Drugs :
• k+ sparing diuretics
• ACE inhibitors
• Cyclosporine
• K+ salt of penicillin
Excessive intake
• Table salt substitute
• Vegetarian ( juices)
• Old blood transfusions
Endocrine:
Addison’s
Shift of k+ : Acidosis
Familial periodic paralysis
Release of k+ from tissue
⁃ Rhabdomyolysis
⁃ Severe Burn
⁃ Haemolysis
⁃ Tissue injury
⁃ Cytotoxic therapy
Spurious:
⁃ prolonged use of to tourniquet
⁃ Haemodialysis of blood samples
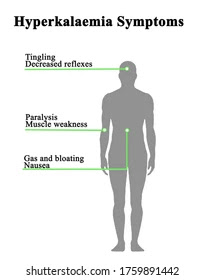
Clinical presentation
• History of intake of K+ sparing drugs
• Cardiac arrhythmias
• Muscles weakness
• Abdominal distension
• Hypoventilation
• CNS
⁃ Drowsiness
⁃ Confusion
⁃ Coma
• Endocrine
⁃ Increased Aldosterone
⁃ Increased release of Noradrenaline
Investigations
Blood : serum electrolytes
Na+ , K + ( >6.5mmol/ L)
ECG :
⁃ Tall tented T- wave
⁃ Prolonged p-R wave
⁃ Widening of QRS - Complexes

Management
⁃ Identify and treat underlying cause
⁃ Avoid food rich in K-
⁃ Avoid K+ sparing diuretics
(a) 10 ml calcium gluconate 10% iv. Over 10 min repeated as necessary if severe ECG changes . This provide cardiac protection, it doesn’t change K + level in serum.
(b) Insulin + glucose
20 unit soluble insulin + 50 ml of glucose 50% iv infusion or 8 Units insulin in 500 ml of 5% dextrose.
It will shift k+ into cells and decreased serum level of potassium. Monitor plasma K+ after 20-30 min and repeat if necessary. Start infusion of 10-20% dextrose 500 ml 4-6 hourly ( to minimize rebound K+)
(c) if metabolic acidosis is present- infuse sodium bicarbonate 1.26 % 500 ml 6-8 hourly until plasma HCO3 is normal.
(d) Nebulized salbutamol or alternative salbutamol: 0.5 mg iv. in 5% over 15 min .
(e) polystyrene sulfonate resin : 15 gm *8 hourly in water orally, if vomiting used enema 30 gm. Follow by colonic irrigation to remove k+ from the colon . Each gram of calcium resonium binds 1 mmol of potassium.
(F) Consider dialysis in patients who have not responded to medical treatment.
Dialysis : Haemodialysis
Peritoneal dialysis
(g) Treat underlying primary causes
# Important question are :
1. How does hyperkalemia affect the body ?Ans : Hyperkalemia is a higher than normal level of potassium in the blood. Although mild cases may not produce symptoms and may be easy to treat, severe cases of hyperkalemia that are left untreated can lead to fatal cardiac arrhythmias, which are abnormal heart rhythms.

2. What happens when your potassium is high?
Ans :Having too much potassium in your blood can be dangerous. Potassium affects the way your heart's muscles work. When you have too much potassium, your heart may beat irregularly, which in the worst cases, can cause heart attack.

Hypokalaemia
When the serum potassium level falls below 3.5 mmol/ l is called hypokalaemia . If level < 2.5 mmol / l , it requires urgent treatment.
Causes :
GI tract loss :
⁃ Diarrhoea and vomiting
⁃ NG Aspiration
⁃ Mucus secreting large bowel neoplasm
Loss from the kidney:
• Hormonal :-
⁃ corn’ s disease
⁃ Cushing ‘s syndrome
⁃ Corticosteroids therapy
⁃ Secondary hyperaldosterone
• Drugs
⁃ Diuretics
⁃ Carbenoxolone
⁃ Steroids
⁃ Ions exchange resins
⁃ Amphotericin B
• Primary Renal disease
⁃ Recovery phase of ATN
⁃ Relief obstruction
⁃ Interstitial Nephritis
⁃ Renal tubular acidosis. ( Type l,ll ,lll)
• Anabolic state of the body :
⁃ Insulin therapy
⁃ Hyperalimentation
⁃ Active bone marrow
• Shift or K+ from extracellular compartment
⁃ Alkalosis
⁃ Insulin therapy
⁃ Familial periodic paralysis. ( Hypokalaemia)
• Decreased K+ intake
⁃ Hypokalaemic diet
Clinical presentation
⁃ Malaise and weakness
⁃ Cardiac : Arrhythmia
⁃ Hypotonia
⁃ Muscles cramps and tetany
⁃ Hyporeflexia
⁃ Muscles weakness
⁃ Postural hypotension
⁃ Abdominal distension with decreased
⁃ Enhanced digital toxicities .
Investigations:
Blood: serum level <3.5 mmol/ l
ECG :
⁃ prominent U- wave
⁃ Flat T- wave
⁃ ST - depression
⁃ Evidence of arrhythmias
Urinary k+ < 20 mmol/day excludes renal loss and > 30 mmol/ day is suggestive of renal loss.
Management:
Therapeutic goals :
⁃ prevent life - threatening complications.
⁃ Correct the potassium deficit .
⁃ Minimize ongoing losses .
⁃ Treat the underlying causes.
1. Replacement k+ : potassium chloride: Oral or IV infusion.
2. Mild asymptomatic: Oral potassium supplementation
3. Severe symptomatic : Intravenous KCL infusion 40 mmol kCL in normal saline over 4 hours.
( 10 mmol/ hr , maximum rate should not be exceed 20 meq/ hr.)
4. Monitor plasma potassium every 4 hours .
5. Continue IV potassium until normal level is attained.
Calculation :
( Normal k+ -observe k+ level ) * 0.5 of body weight.
50 mmol per day or 1 mmol per kg per day .)
1 ampoule: 10 ml KCL contain 20 mmol / l
Infusion rate not more than 20 mmol / l and concentration not more than 40 mmol/ l.
II. Treat underlying cause of hypokalaemia :
⁃ Stop diuretics or replace with potassium- sparing diuretics
⁃ Stop laxatives
⁃ Supplement potassium intake .
Some important question:
1. What can happen if your potassium level is too low?
Ans :A low potassium level has many causes but usually results from vomiting, diarrhea, adrenal gland disorders, or use of diuretics. A low potassium level can make muscles feel weak, cramp, twitch, or even become paralyzed, and abnormal heart rhythms may develop.
2. How do you fix low potassium?
Ans :Potassium supplements are generally prescribed for low potassium levels. If the situation is severe, potassium might be given as an intravenous (IV) solution. If there is a condition that causes the hypokalemia, such as low levels of magnesium or an overactive thyroid, the other condition must be treated also .
Thanks for visiting our blog spots 🙏
If you need any note of CTEVT related faculty
Then contact us :
Facebook : https://www.facebook.com/CTEVT-TECHnical-NEPAL-103116595350525/
Gmail: ctevtechnical@gmail.com
# stay connected with us .
Post a Comment
If you have any doubts please let us know .